Current and potential future therapies for CDKL5 ...
Most current treatment options for CDKL5 are aimed at the related symptoms. So, we see treatment to try to improve seizures, managing reflux, and various therapy modalities for improving motor function and cortical visual impairment. At the moment there are no treatment options available to address the underlying cause of the disorder although there is on-going research. On this page I have summarised available treatments for the symptoms of CDKL5 as far as they are established, as well as reviewing potential strategies for treatment of the underlying cause of the disorder.
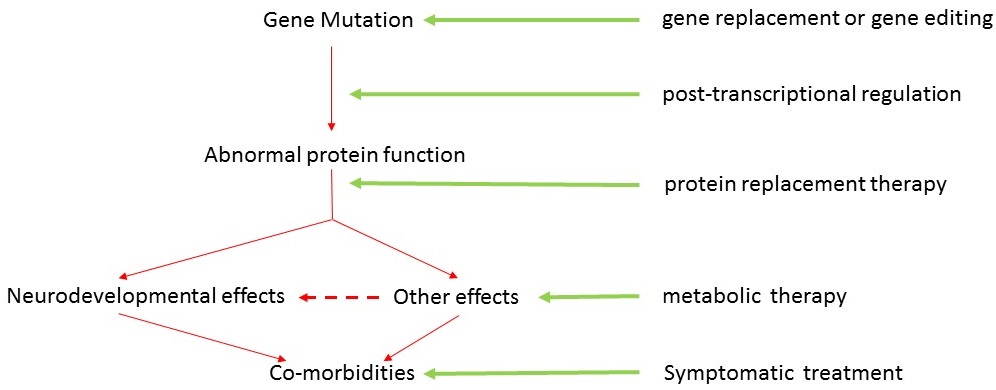
Strategies for treating the CDKL5 Disorder
This is an overview of the pathway from CDKL5 gene to protein function. You can see that there are various points from gene to target where potential treatments may act.
Gene Therapy
There are a number of techniques now under investigation. The first is gene replacement. The principle of gene replacement is very straight forward, replace the mutated gene with a normal one – simple!! In practice of course this is highly technical stuff. Basically the correct gene is introduced into the brain using something called a “vector” which is usually a virus. The virus (vector) carries the correct gene into the brain and is then able to transfer the gene into neurons of the brain. Very little has so far been done with CDKL5. However, a considerable amount of work has been done with MECP2 (Rett) in mouse models, so techniques are being developed. Reference
Other techniques are being researched including the use of something called naked DNA. As far as we know, CDKL5 is caused by mutations in a single gene and so would be very suitable to gene replacement – in contrast to other conditions which are associated with abnormalities in more than one gene. However, there are a number of hurdles that need to be overcome before gene replacement can become a reality for us. An appropriate and effective vector has to be established, the gene has to get to the right part of the brain and it needs to then be functional – that is go on to produce the CDKL5 protein in the right way. Gene replacement therapy for CDKL5 is in its very early days.
Other forms of gene therapy such as gene editing are in their early stages.
Post-transcriptional regulation
You will recall that the gene is read (transcription) to produce RNA and that this then acts as a template to produce the protein through translation. The initial RNA produced by transcription undergoes considerable modification and regulation before being translated to produce the final protein.
This has opened up a whole field of study into whether this post-transcriptional regulation can itself be altered in favour of reducing the effects of any mutation. It is hoped that research will lead to the development of new “small molecule” drugs that may achieve this. However, there is also research being undertaken into the effect other more well established drugs might have on the same post-transcriptional pathways - so called drug repurposing. Drugs are developed for a particular reason because of a specific physiological effect that they have. So, antibiotics have a specific effect on bacteria and are therefore used to treat bacterial infections. However, the same drug may also have a second effect on a different system, which may be of value – and there are now some drugs that have been shown to affect post-translation regulation. The advantage here is that these drugs will already have been through a development and safety testing programme and so it should be a much shorter process to get them into clinical use. Many drugs have already been through this process for a number of different conditions - Link
Much excitement has been generated by the development of a drug called “Translarna”. In the situation where you have a missense mutation producing a premature “stop” codon, the subsequent protein will be abnormally short which will obviously affect its function. Translarna prevents the “stop” codon being read so that the full length of the transcript is read and a protein is produced of relatively normal length. Research has been undertaken for its use in Duchenne muscular dystrophy and cystic fibrosis. Reference
Protein Replacement Therapy
Protein Replacement Therapy (PRT) is also a relatively new and expanding field and potentially offers us some hope for the treatment of CDKL5. The technique involves the introduction of a protein that is deficient, so as to replace the loss of function that that protein deficiency causes. The principle is established in that it has been shown in mouse models that an injected protein can retain its biological activity. The detail of the technique, however, is still to be developed and perfected.
One obstacle is the method by which the protein is introduced. Proteins that are injected into the bloodstream may be metabolised before they get anywhere near their target organ (such as the brain in the case of CDKL5). The blood-brain-barrier itself will stop most things getting through anyway. There are some conditions - like Parkinson’s disease - where the deficiency is sufficiently localised that implanting the protein directly into the brain at the affected area might be feasible. Unfortunately with CDKL5 the deficiency of the CDKL5 protein is likely to be widespread throughout the brain so other techniques of introducing the CDKL5 protein need to be developed. Mouse models have involved injections into the abdominal cavity.
The production of the CDKL5 protein itself also seems to be an issue. Host cells are used to achieve this and the commonest host cell is E.Coli because it can produce large quantities of protein. Unfortunately it seems that that the CDKL5 protein is not compatible with E.Coli so other less efficient cell lines are being investigated…just our luck...!!! Many of these problems are being addressed and so approved human trials may not be too far away although there may well be a number of hurdles still to be overcome before the technique is perfected.
Metabolic Therapy
A number of studies examining the molecular pathways in which the CDKL5 protein is involved have suggested the potential for further therapeutic strategies. I have highlighted a few here but I am sure more will become evident as further studies are produced.
AKT/GSK-3β signalling pathway - Research suggests that the CDKL5 protein acts through something called the AKT/GSK-3β pathway, and that this pathway is somehow disrupted in CDKL5. Some further research in mice models has shown that by “correcting” the disruption to the AKT/GSK-3β pathway, the histological and behavioural changes associated with CDKL5 can be improved. Abstract and Review
Insulin-like Growth Factor 1 (IGF-1) is a protein also involved in the AKT signalling pathway. IGF-1 itself is not thought to be deficient in CDKL5. However, it has been shown, again in KO mice, that the addition of extra IGF-1 can cause the reversal of defects seen in CDKL5. Abstract and Review
Oxidative stress - There has been some research that has suggested that children with CDKL5 may be prone to both abnormal cholesterol regulation and oxidative stress. These biochemical abnormalities are common to both CDKL5 and Rett syndrome and may reflect the overlap in molecular pathways affected in the 2 conditions. Research is at a very early stage but if there is a significant problem in CDKL5 with cholesterol regulation and oxidative stress then this may have implications for new treatment strategies. Abstract and Review
ω-3 PUFAs - So, CDKL5 is assumed to be primarily a neurological condition. However, the argument is that there may also be secondary effects contributing to the phenotype through oxidative stress and related free-radical damage. Treatment with ω-3 PUFAs may therefore go some way to reducing these secondary effects but presumably would not affect the primary underlying neurological condition. What may not be clear, however, is how much of a child's phenotype is related to the direct consequences of the underlying genetic disorder as opposed to the secondary effects, including the effects of oxidative stress. This is obviously still a very exciting piece of research for families with children particularly with Rett syndrome where more research has been done. Text and Review
I have reviewed more of these as the research becomes available - see CDKL5 research page - annual reviews.
Seizures
Seizures are clearly a big problem in CDKL5. The majority of affected children start having them within the first few weeks or months of life. Their pattern often changes and evolves with age. In many cases, seizure control proves difficult to maintain with conventional anti-epileptic drugs or other types of treatment (ketogenic diet, VNS). Reference
There has also been a lot of interest in the medical use of marijuana. There are 2 substances which have been found helpful in certain cases. Hemp and marijuana both belong to the Cannabis plant genus. Hemp differs in that it has very little tetra hydro cannabinol (THC) and higher amounts of cannabidiol (CBD) High amounts of THC are associated with marijuana’s well-known euphoria. CBD is not. Proponents of hemp oil treatment say that users don’t feel stoned. Link
GI Disorders
Studies have shown that GI problems are common in CDKL5. Families are having to cope with these issues on a day to day basis and there is some evidence that they do not always get the support they need from their healthcare professionals. Upper GI problems including reflux are common. Ultimately there can be a role for surgery to try and correct reflux although there is much that can be done before this.
Sleep Disorders
Sleep is a big issue for many children, and young adults, with CDKL5. There is unfortunately not enough known about the underlying mechanisms for sleep disturbance in CDKL5 to know how to deal with it. Is it seizure activity, pain,a simple circadian rhythm issue or what..? There is but one study / review and usually the message is around good sleep hygiene. Unfortunately, as I once pointed out at a CDKL5 Forum, many parents are sleep hygiened up to their streaky red eyeballs. I think much research is need here...
Cortical Visual Impairment
I don't imagine many if in fact any of us can really understand what it would be like to have CVI. There has been a nice survey of parents on the subject and there is also a nice review from The Cerebral Visual Impairment Society.
Other comorbidities
As time goes by, the various symptoms and comorbidities associated with CDKL5 are becoming better understood. Most affected families will already have experienced these problems - particularly sleep problems and GI disturbances - and these are slowly being recognised and described in the scientific literature. Hopefully as healthcare professionals become more aware of these issues then more interest will be generated in trying to help families manage these day to day problems. Reference